Introduction
Tennis is widely considered as an asymmetrical sport with great unilateral predominance (Cools et al., 2014; Sanchis-Moysi et al., 2009, 2010, 2011). Because of the way it is played, functional and morphological differences appear as a consequence of prolonged exposure. Structurally, bone mineral density, hypertrophy and fiber type distribution can report significantly greater values in one side of the body when compared to the opposite (Sanchis-Moysi et al., 2009, 2010, 2011, 2017). In the same way, these differences also appear when comparing neuromuscular performance, strength values (Fernandez-Fernandez et al., 2019; Sanchis-Moysi et al., 2009) and range of motion (ROM) (Fernandez-Fernandez et al., 2019; Moreno-Pérez et al., 2016) outcomes. When assessing strength values specifically, asymmetries appear clearly around the shoulder (Cools et al., 2014; Fernandez-Fernandez et al., 2019; Gillet et al., 2017; Moreno-Pérez et al., 2015), the hip (Moreno-Pérez et al., 2017) and lumbo-pelvic muscles (Sanchis-Moysi et al., 2010, 2017). These differences have often been associated to an increased risk of injury prevalence. For example, considering the shoulder complex, a deficit in glenohumeral internal rotation ROM with respect to the contralateral side of the body (GIRD) increases likelihood of shoulder or elbow pathologies (Moreno-Pérez et al., 2015; Shanley et al., 2011). Opposite to this, bilateral differences could not be observed in lower body structures such as the hip, expressing compromised mobility around the joint, but no significant variances in side-to-side values (Moreno-Pérez et al., 2016; Young et al., 2014). Moreover, strength imbalances present at the rectus abdominis seem to be relevant regarding lower back pain and muscle tears (Sanchis-Moysi et al., 2010, 2017), establishing the importance of contralateral ROM, strength ratios and differences.
In the same way, muscle mechanical characteristics, especially stiffness, have previously been studied in relation to their importance regarding performance and the link to injury in a wide range of sports (Brazier et al., 2019; Pickering Rodriguez et al., 2017; Pruyn et al., 2012, 2015). Concerning effects on performance, specifically in tennis, a certain level of stiffness may interpose or aid in velocity production of strokes, depending on the structure analyzed (Colomar et al., 2020). Interestingly, this idea follows previous statements on how stiffness may be an important factor benefiting performance and associating greater values to enhanced sprinting or jumping (Brughelli and Cronin, 2008). Counterproductively, an increased level of these capacities could also result unfavorable and contribute to increased shock peak forces, reduced ROM (Brazier et al., 2019) and a high level of muscle tightness (Marcondes et al., 2013), which, as seen in overhead athletes (Moreno-Pérez et al., 2015), can generally lead to pathologies or injury. Furthermore, it seems that a high level of asymmetry of stiffness values when comparing limbs could also be directly associated to injury risk and worsen the performance outcome (Pruyn et al., 2012). As pointed out in previous works in other sports (Pickering Rodriguez et al., 2017), an optimal stiffness zone that benefits performance variables and does not interfere or increases injury likelihood is yet to be further investigated, but the importance of side-to-side ratios seems clearly relevant regarding performance and injuries. Due to the aforementioned characteristics, the hypothesis tested here was that the dominant upper extremity of tennis players would show significantly greater values of stiffness, tone and time to relaxation compared to the contralateral side of the body, as chronic adaptation to high volumes of tennis practice.
No studies to our knowledge have assessed interlimb asymmetries regarding mechanical muscle characteristics in young tennis players. Therefore, and because of the aforementioned asymmetric nature of tennis and its possible negative outcome or implications for training, it seems interesting to value side-to-side differences concerning muscle mechanical characteristics. Thus, the goal of this study was to assess interlimb asymmetries regarding tone, stiffness, elasticity and time to relaxation in young tennis players.
Methods
Participants
Thirty-four male tennis players (mean ± SD; age, 16.7±1.2 years; body height, 1.78±0.07m; body mass, 70.3±6.4kg; BMI, 22.1±1.3kg/m2) with an International Tennis Number (ITN) ranging from 2 to 4 (advanced level) participated in this study. This sample size was justified by a priori power analysis conducted in G∗power using a target effect size (ES) of 0.5, alpha level of 0.05, power of 0.80 and two tails, which determined that 34 subjects would be needed for participation (G-Power software version 3.1.9.5, University of Dusseldorf, Dusseldorf, Germany). The player’s ITN was established by the consensus of three coaches accredited with RPT (Professional Tennis Registry) level 3, following the ITN Description of Standards (www.internationaltennisnumber.com) Thirty-one of 34 (91.2%) subjects performed a two-handed backhand and 8.8% of participants were left-handed. Players had a training volume of 25 h·week-1 of which 5h accounted for fitness training and 20h for technical and tactical sessions. The mean training background of players was 7.8±1.8 years, which focused on tennis-specific training (i.e., technical and tactical skills), aerobic and anaerobic training (i.e., on- and off-court exercises), and strength training (which included prevention strategies in the form of foam rolling, static stretching and posterior shoulder capsule muscle strengthening exercises). Inclusion criteria for all subjects required each participant to have a minimum of 1-year experience in strength training and 5 years of tennis training and competition. Participants were excluded from the study if they had a history of upper or lower extremity surgery, shoulder, back or knee pain and/or rehabilitation for the past 12 months. All subjects were informed in advance about the objectives of the study and, before participation, players or their legal tutors voluntarily signed an informed consent form. The study was conducted research with human beings, established in the Declaration of Helsinki of the AMM (2013) and approved by an accredited Ethics Committee.
Design and procedures
This was a cross-sectional laboratory study with uninjured participants. The collection of data took place in March and April during normal in-season training weeks in groups of 4 or 5 players, executed from 8:00 to 8:30 am, before players’ normal technical-tactical training and prior to any physical activity or warm up routines. Participants had not trained for at least 16 h before the testing procedure. During testing, participants were assessed for mechanical muscle characteristics via muscle natural oscillation (Dm) using a hand-held myometer. The use of pain-relieving strategies (e.g., foam rolling or massage) or energy techniques was not allowed during tests as well as stretching exercises on the same day in order to avoid interferences with the results.
Measures
Contractile properties measurement
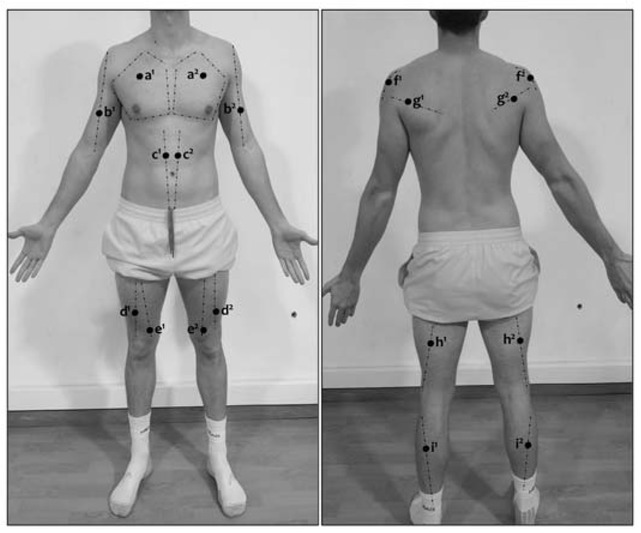
Muscle properties, which involved tone (mechanical tension in a relaxed muscle), stiffness (the resistance of the muscle to an external force that changes its initial shape), elasticity (recovery of the muscle’s initial shape after contraction or removal of an external force) and time to relaxation (time for the muscle to restore its initial shape after external force) (Ko et al., 2018) were measured on both the dominant and the non-dominant side of the body using a hand-held myometer (Myoton-Pro, Myoton AS, Tallinn, Estonia) following previous similar protocols (Colomar et al., 2020) and approximately in positions marked in Figure 1. The dominant extremity or side of the body was established based on upper body dominance (i.e., extremity used to hit strokes). Although this may not match when referring to the lower body, for this study, a right-handed player would have a dominant right leg and vice versa, since leg dominance does not seem relevant in specific tennis actions. Before the assessment, body marks were established for nine measurement points using the SENIAM electrode placement guidelines (Hermens et al., 2000). The muscle groups chosen were those mostly involved in tennis strokes (Chow et al., 2009; Girard et al., 2005; Kibler et al., 2007; Rogowski et al., 2011) attending to the whole kinetic chain, i.e., the infraspinatus (I), deltoids (D), rectus abdominis (RA), the rectus femoris (RF), vastus medialis (VM), biceps femoris (BF) and the lateral head of the gastrocnemius (G). Since the goal of this study was to assess chronic adaptation in the form of variations of muscle mechanical characteristics, measurements were performed with a state of muscle relaxation and participants lying down (RA), seated (PM, B, I, D) or in an anatomical position (RF, VM, BF, G), depending on the test point. The tip of the Myoton-Pro was placed perpendicular to all measurement zones sampling at 15ms with a force of 0.58N and measured the damped natural oscillations caused by the probe impact. The device's accelerometers operated at 3200Hz, offering an average value of 5 consecutive measurements. The Myoton-Pro reliability shows excellent test-retest values as shown previously in other investigations (Colomar et al., 2020).
Statistical analysis
Descriptive data were reported as mean ± standard deviation (SD). The normality of the distributions and homogeneity of variances were assessed with the Shapiro-Wilk test. Parametric and non-parametric statistics were used when appropriate. The differences between group mean values of the dominant and the non-dominant side were tested by a paired t-test, in cases of non-normality the nonparametric Wilcoxon paired test was used to assess differences. The magnitude of the differences in mean was quantified as effect size (ES) and interpreted according to the criteria used by Cohen (1988); <0.2=trivial, 0.2–0.4=small, 0.5– 0.7=moderate, >0.7=large. The level of significance was set at p<0.05. All statistical analyses were performed using SPSS 26.0 software (SPSS Inc., Chicago, IL, USA).
Results
Inter-limb differences for stiffness, tone, elasticity, and time to relaxation are presented in Figure 2, while values for assessing the magnitude of changes and effect sizes are shown in Table 1. Significant differences and small-to-moderate effect sizes for greater stiffness and tone were found for the dominant biceps femoris (-11.1% and -5.6%; ES=0.53 and 0.54) and the non-dominant vastus medialis (5.4% and 3.2%; ES=0.33 and -0.41), while greater tone was present in the non-dominant pectoralis major (4.0%; ES=-0.56). Time to relaxation was increased in the dominant biceps femoris (10.3%; ES=-0.58), the non-dominant pectoralis major (5.1%; ES=-0.56) and the gastrocnemius (9.1%; ES=-0.5). The non-dominant infraspinatus and the dominant rectus abdominis showed greater elasticity than contralateral muscles (9.9% and -8.0%; ES=-0.58 and 0.6, respectively).
Figure 2
Dominant and non-dominant differences regarding stiffness (A), tone (B), elasticity (C) and time to relaxation (D).
B=biceps brachii; I=infraspinatus; D=deltoid; PM=pectoralis major; RA=rectus abdominis; RF=rectus femoris; VM=vastus medialis; BF=biceps femoris; G=gastrocnemius; †=significant differences from the dominant limb at p<0.05.
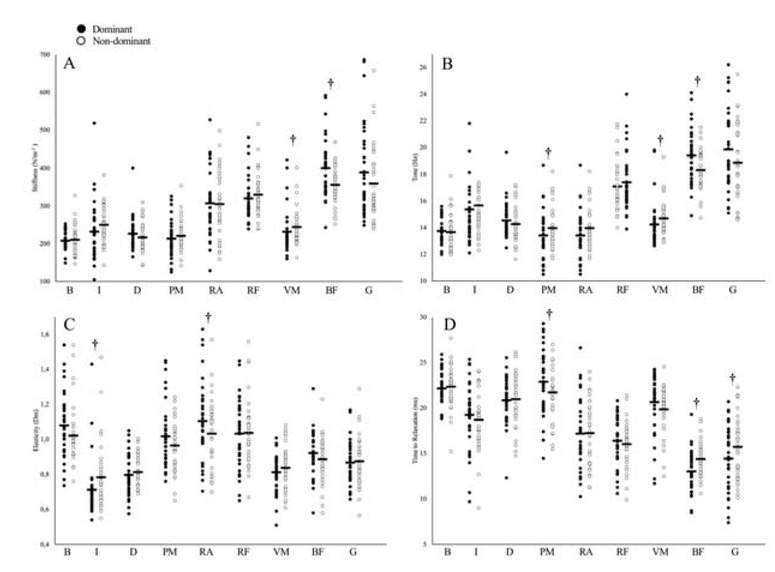
Table 1
Dominant and non-dominant stiffness, tone, elasticity, and time to relaxation differences (n = 34).
Discussion
The main finding of this study was that although certain differences regarding muscle mechanical characteristics existed when comparing side-to-side values in youth tennis players, these did not seem to present a consistent outcome or happen in more muscle groups. Regarding the lower body, significant (p<0.05) moderate differences towards increased stiffness, tone and time to relaxation (-11.1%, -5.6% and 10.3%; ES=0.53, 0.54 and -0.58, respectively) could be observed in the dominant biceps femoris. Besides this, only small variations towards increased stiffness and tone in the vastus medialis (5.4% and 3.2%; ES=-0.33 and -0.41) and the time to relaxation of the gastrocnemius (9.1%; ES=-0.5), both on the non-dominant side, were registered. Upper body assessment followed this line and small differences towards greater values in tone and elasticity were observed only in few muscle groups such as the non-dominant pectoralis major (5.1%; ES=-0.56) and infraspinatus (9.9%; ES=0.58) and the dominant rectus abdominis (8.0%; ES=0.6). Although previous investigations have well established the existence of stiffness asymmetries among athletes, even with significant relations to soft-tissue injury risk (Pruyn et al., 2012), these differences account for lower body musculature and have typically measured active stiffness levels via hopping tests (i.e., vertical stiffness). When assessing passive measurements as in this study, investigations have found certain asymmetries in some muscle groups, although conclusions were drawn indicating that these indexes may not be as indicative or present the same differences (Pruyn et al., 2015). Elevated levels of stiffness have been thoroughly related to enhanced performance indicators such as strength, the rate of force development and jumping values (Pruyn et al., 2012, 2015), all of which are relevant to tennis performance, but also represent dynamic actions that may be better addressed using measurements which assess an active state of the muscle. It could be that, as increased levels of stiffness and derivative muscle properties (i.e., tone, time to relaxation and elasticity) are related to a faster release of elastic energy and are therefore advantageous for highly dynamic explosive actions, adaptation is not evident when analyzing the muscle in a relaxed state. Nevertheless, changes and asymmetries derived from high volumes of tennis training and match-play have previously been observed in the form of morphological (Sanchis-Moysi et al., 2009, 2010, 2011, 2017) and neuromuscular (Madruga-Parera et al., 2019) chronic adaptation. A possible explanation to rather small differences between side-to-side muscles could be that more evident asymmetries appear as age, level and consequent training volumes increase. Differences have previously been observed in players at prepubescent ages (Sanchis-Moysi et al., 2017), although greater differences when comparing muscle volumes appear when analyzing professional subjects (Sanchis-Moysi et al., 2009, 2010) with similar weekly loads, but greater training experience than participants in this study. Therefore, years of competitive training and competition could be a determining factor affecting side-to-side asymmetries.
Regarding results registered for the lower body, significantly greater values and small-to-moderate changes for stiffness, tone and time to relaxation could be observed for the dominant biceps femoris. In tennis, a great deal of short sprints are performed during play, covering short distances that average 5 to 15 m per point and 20% of these tending to follow horizontal displacement (Galé-Ansodi et al., 2017). In the acceleration phase of sprinting, the biceps femoris shows high electromyographic (EMG) activation, especially in the swing phase (Morin et al., 2015), and thus it would be reasonable to assume this musculature would show trends towards increased levels of stiffness, tone and consequently time to relaxation, even in resting conditions as chronic adaptation. Nevertheless, results here indicate differences within the contralateral side of the body rather than an increased level of activation. Coordinatively, when accelerating to sprint, athletes tend to perform a step back movement in order to accelerate and move forward as fast as possible, taking advantage of the stretch shortening cycle (SSC) and ground reaction forces (Frost and Cronin, 2011). This step back is normally repeatedly performed with the same leading leg, simply due to the convenience and the habit of the player. The combination of repetitive short forward accelerations added to the high activation of the biceps femoris when swinging the leg forward in sprinting could explain higher values observed. Regarding the vastus medialis and gastrocnemius, the importance of these muscles is evident during the serve, especially in the forward leg (i.e., non-dominant here) at the end of the concentric (Girard et al., 2005) or the landing phase, respectively. Although with caution and being speculative, the high volume of serving during practice and match-play (Perri et al., 2018) could place a higher degree of stress over both muscle groups of the non-dominant leg and increase stiffness and tone differences when compared to the contralateral side. Also, side-step acceleration patterns are preceded usually by players performing split steps, which generate high levels of activation of the gastrocnemius on the opposite direction of movement before and after landing (Uzu et al., 2009). This contributes to stiffness regulation during the subsequent jump, producing an effective and quick lateral first step (Uzu et al., 2009). Moreover, the vastus medialis behaves as a stabilizer muscle (Brown et al., 2014) in side breaking and accelerating movements. These actions account for 70% of total volume during tennis match-play (Galé-Ansodi et al., 2017), in many occasions in order to hit a baseline forehand, as it seems to be the most repeated stroke, especially when referring to male junior tennis (Kovalchik and Reid, 2017). This is important due to the laterality of these specific tennis actions. To hit a forehand, players typically have to side-shuffle towards the doubles isle, which is at the same side of their dominant extremity. This means the outer leg (i.e., non-dominant here) performs the push off motion in order to move towards the hitting position. In any case, this is speculative, and results seem to indicate small differences in few muscles tested and active measurements may be a better option to assess side-to-side asymmetries.
Regarding trunk and upper body values, side-to-side differences were found regarding tone of the pectoralis major, with a greater value in the non-dominant extremity when compared to the playing arm. Results here are surprising regarding the repetitive internal rotation, horizontal adduction and scapula protraction motion of the dominant extremity, especially when playing serves and forehands (Cools et al., 2014). Typically, players present adaptation due to these actions in the form of posterior capsular tightness, rotator cuff strength imbalances and scapular dyskinesis (Cools et al., 2014), preceded by alterations in length in muscles such as the pectoralis minor (Cools et al., 2010). It would be expected that, contrary to the results, higher values of stiffness and/or tone, even in resting conditions, would be found in the dominant pectoralis major as adaptation to its high activity during strokes (Rogowski et al., 2011) and response to fatigue (Macgregor et al., 2016). The greater level of tone in the non-dominant muscle found here may have two reasons. First, due to the aforementioned increased activation of the pectoralis major during main strokes, fatigue appears sooner and the central nervous system triggers adaptation performing different neuromuscular adjustments and compensatory strategies to overcome fatigue and conserve performance (Rota et al., 2014), resulting in significant differences when compared to the contralateral side of the body. Second, fitness training interventions of the participants tested here included a great deal of stretching and foam rolling exercises. These programs were performed daily, especially in the dominant extremity, and aimed to decrease injury likelihood reducing shoulder capsule tightness using strategies such as self-myofascial release. As stated in the literature, these techniques can achieve progressive reduction in muscle stiffness and tone, being of greater magnitude when observed after a certain period of time (Behm and Wilke, 2019). Training programs including self-myofascial release and performed regularly by players mainly on the dominant extremities may explain side-to-side differences in this matter and limit findings as this variable was not registered. Concluding, the non-dominant abdominal and dominant infraspinatus presented lower elasticity values, or capacity of the muscle to recover its initial shape (Ko et al., 2018). Elasticity is measured via an oscillation decrement (Dm), which is inversely proportional to elasticity, meaning a greater Dm results in a lower capacity of the muscle to return to its original form. Due to the tennis serve motion, the rectus abdominis presents greater hypertrophy on the non-dominant side of the athlete’s body (Sanchis-Moysi et al., 2010). Because of repetitive contractions, this muscle activates asymmetrically and is therefore responsible for this adaptation (Sanchis-Moysi et al., 2010). Unilateral repetitions most likely predispose to greater stress and could present greater Dm values, meaning that fatigue, repetitive loading and stress inhibit effective recovery of the muscle. In the same manner, the dominant infraspinatus could be affected by match-play and competition, especially during the follow-through phase of the serve to help control humeral deceleration (Kibler et al., 2007). As a possible reason no differences could be observed in further upper body contractile variables, the fact that the majority of players played a two-handed backhand (91.2%) could affect results. EMG activity of the deltoids, pectoralis major, biceps and triceps brachii muscles during the two-handed backhand is higher in both limbs than executing in the one-handed fashion (Genevois et al., 2015). Due to this, differences would be diminished as muscle participation is similar on both sides when performing this specific stroke.
As a perspective for future investigations, although this study found slight asymmetries in some muscle groups as adaptation to tennis practice and match-play, the analysis of data regarding musculature in an active state could be of great interest. Studies such as that of Pruyn et al. (2016) state correlations between the use of myometry and active stiffness measurement methods such as vertical hopping tests, indicating the possibility of using these methods for further insights into the matter. This study had some limitations. Although only two participants (8.8% of total) performed a one-handed backhand while playing, effects on muscle characteristics could differ highly when compared to the two-handed fashion. As stated in previous research (Genevois et al., 2015), disparities regarding muscle activation and kinematic differences between both styles may affect mechanical muscle adaptation and outcomes, hence affecting to some extent results of this study. Last, the periodic use of self-myofascial release techniques by players involved in the investigation could somewhat affect results.
In conclusion, moderate differences regarding muscle properties can be observed in the dominant biceps femoris of young tennis players. Also, small differences towards an increased level of stiffness and tone seem to appear in the non-dominant vastus medialis and pectoralis major, while greater time to relaxation and elasticity values are present in the non-dominant gastrocnemius, infraspinatus and dominant rectus abdominis, respectively. These measurements reflect to some extent the existence of differences when comparing side-to-side values in young tennis players, however, passive measurements of a relaxed muscle using a hand-held myometer do not seem to fully represent possible adaptation and changes derived from training and gameplay.