Introduction
Indoor sport climbing has experienced an increase in its popularity in both recreational and competitive terms, with its first participation in the Olympic Games in Tokyo 2021. This has led some researchers to focus on the analysis of the possible relationships between climbing performance and anthropometric (Grant et al., 2001; Watts et al., 1993), biomechanical (Bourdin et al., 1998; Quaine et al., 1997) and physiological (Bertuzzi et al., 2007; Magiera et al., 2018; Mermier et al., 2000) variables. Previous findings suggest that maximal upper limb strength is a key factor for successful climbing performance (Mermier et al., 2000), with particular relevance for finger flexors (Magiera et al., 2013; Michailov et al., 2018). It has been demonstrated that well-trained climbers possessed a higher handgrip force (Quaine et al., 2003) and a higher activation of the flexor digitorum superficialis (FD) when compared with non-climbers during a pull-up climbing movement (Koukoubis et al., 1995). These neuromuscular adaptations have been attributed to high-intensity isometric forearm muscle contractions often performed by climbers during ascents of climbing routes (Baláš et al., 2015; Michailov et al., 2014).
The relevance of handgrip force for sport climbing performance has been established through evaluation based on traditional and adapted handgrip dynamometry (Quaine et al., 2003; Thompson et al., 2015), which involves a certain financial cost and the need for specialized evaluators. Those characteristics of evaluation may restrict the number of climbers who may have access to the measurement of specific maximal handgrip force, impacting the development of sports training. It is also important to note that, while forearm muscles are required to grip the artificial holds, other muscles of the upper-limbs (i.e., posterior deltoid) are dynamically recruited in order to balance and displace the entire body on inclined walls (Vigouroux et al., 2015). As a possible result, the measurement of strength using traditional or adapted dynamometers is limited by analysing only the forearm muscles, disregarding the importance of other upper limb muscles for climbing performance. Considering these aspects, it would be important to develop new low-cost tools able to assist the measurement of maximal strength of the upper limbs of climbers in a more specific manner.
Therefore, the aim of the present study was to develop a low-cost and easy-to-build tool for measurement of the specific maximal upper-limb strength in rock climbers, named the MBboard. We also described evidence of validity (i.e., construct validity) and reliability (i.e., test and retest analysis) of the MBboard. It was hypothesized that: i) maximum dynamic strength measured by the MBboard (MBboard-1RM) would be able to discriminate between individuals with different levels of rock climbing experience, mainly due to a higher activation of the FD; ii) the performance measured on the MBboard-1RM would be correlated with climbing ability; and iii) the MBboard-1RM would be reliable when analysed in test and retest trials.
Methods
Participants
Ten male rock climbers [rock climbing group (RCG) = 10; age = 28 ± 6 years, body mass 63.7 ± 3.5 kg, body height 175.2 ± 5.1 cm] and ten physically active men [control group (CG) = 10, age = 23 ± 3 years, body mass 72.5 ± 6.3 kg, body height 178.1 ± 6.3 cm] voluntarily participated in the study. The RCG consisted of subjects who were practicing indoor rock climbing for at least 1 year and could climb difficult routes. Self-reported climbing ability was expressed by their higher redpoint grade climbed over the last year and converted to the International Rock Climbing Research Association Scale (Draper et al., 2016) (17 ± 3 IRCRA Scale), similar to a recent study (Michailov et al., 2018). The CG consisted of subjects who were engaged in recreational sports (i.e., jogging, soccer, basketball and cycling) 3-4 times per week for at least one year. As exclusion criteria, participants should not present any cardiorespiratory disease, not be engaged in any medical treatment, not use anabolic steroids, and no suffer from any recent injuries that could compromise their participation. Participants were informed about the risks associated with the study protocol and signed a consent form agreeing to participate in the experiments. This investigation was approved by the Ethics Committee of the University of Sao Paulo for Human Studies (process 2.942.117), in accordance with the Declaration of Helsinki.
Design and Procedures
Experimental design
Participants visited the laboratory on three separate occasions over a 2-wk period, at least 48 hours apart. All tests were performed at the same time of day to avoid the effects of circadian variation. During the first session, participants underwent anthropometric measurements (i.e., body mass and height) and were familiarized with all MBboard-1RM procedures. The MBboard-1RM was performed during the second (i.e., test) and third (i.e., retest) session. During the experimental sessions, maximum strength of the upper limbs and electromyographic activity (EMG) were recorded. Participants were instructed to refrain from exhaustive or unaccustomed exercise, alcohol and caffeine 48-h before the experimental sessions.
Technical characteristics of the MBboard
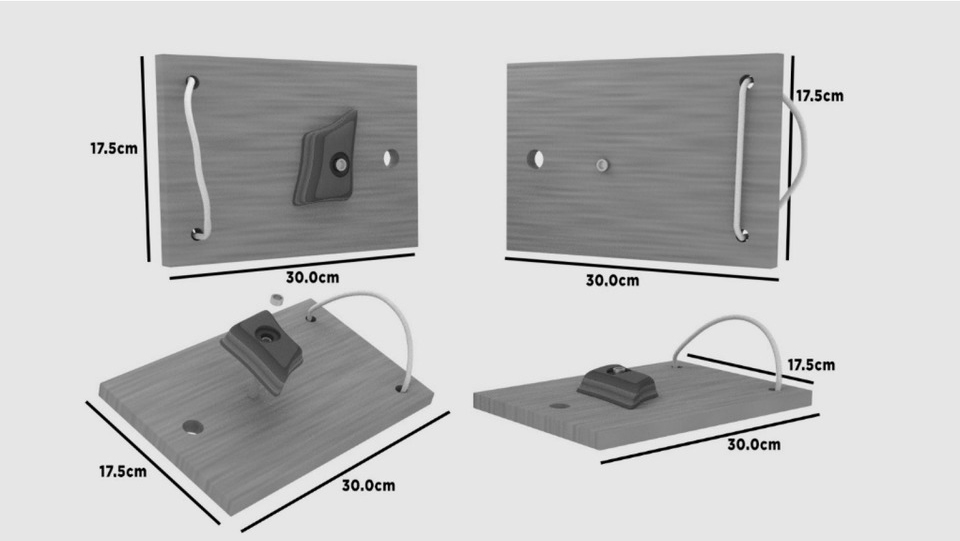
Figure 1 shows a schematic representation of main characteristics of the MBboard. The MBboard is composed of an artificial small climbing hold (with approximately 2.5 cm rounded edge depth)affixed to a wooden board (30 cm length by 17.5 cm width). There is a hole in the wooden board in which a carabiner is placed to connect the MBboard to the crossover machine (or cable- motion strength equipment). On the bottom of the wooden board, there are two parallel holes which serve to place a small cord that surrounds the forearm for the stabilization of the MBboard during exercise.
Maximum dynamic strength measured by the MBboard
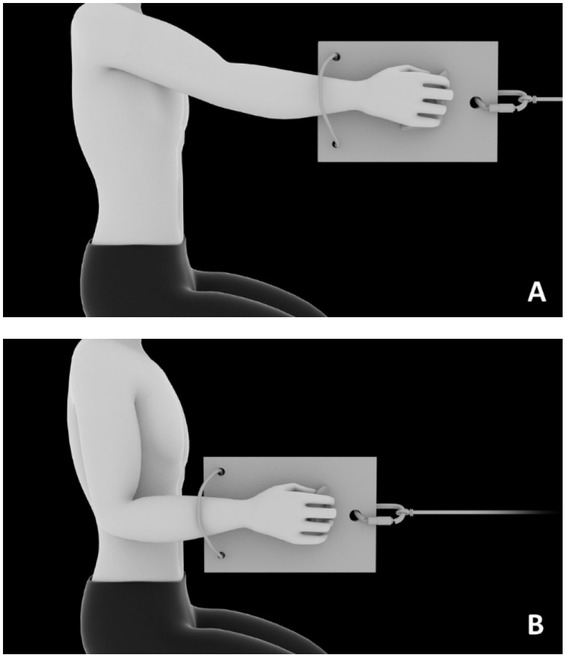
Participants were familiarized with all the procedures, equipment, and proper exercise techniques prior to data collection. An adjustable-height bench press seat was used to keep the knees (90o), trunk (90o), and arms (90o) flexion angles constant during each MBboard- 1RM repetition. At the beginning of each set, participants were instructed to grip the climbing hold and start the MBboard-1RM with the elbow extended and finish it with the elbow flexed at approximately 900during the unilateral seated cable row exercise (Figure 2). The participants’ settings on the crossover machine were recorded to guarantee the same positioning across familiarization and experimental sessions. Participants were free to choose the grip technique during familiarization, which was recorded and replicated in the experimental sessions.
Figure 2
Schematic representation of initial (panel A) and final (panel B) arm positions during MBboard-1RM assessment.
The MBboard-1RM was evaluated on the dominant and non-dominant upper-limb, which was defined based on the subject daily activities (Coley et al., 2008), according to standard procedures for maximum dynamic strength measurement (Brown and Weir, 2001). Participants performed a brief general warm-up composed of a 5-min run at 8 km∙h-1 followed by light upper limb stretching. Following the initial warm-up run, participants performed a specific warm-up composed of three sets, interspaced by a 3-min rest interval. In the first set, five repetitions with the load of 5 kg were performed. In the second set, five repetitions at 50% of the estimated MBboard-1RM were completed. The third set of the warm-up was composed of three repetitions at 70% of the estimated MBboard- 1RM. After the third set, participants rested for three minutes before performing five trials to achieve the MBboard-1RM, which was defined as the maximum weight that could be lifted once using proper technique. A three-minute rest interval of passive recovery was allowed between the attempts. Participants were allowed to use chalk as a natural practice in climbing and the hold was cleaned with a brush when needed. Electromyographic activity (EMG)
During the specific warm-up protocol (i.e., load of 5 kg) and MBboard-1RM measurement, EMG signals were recorded from the right arm. Disposable dual Ag/AgCl snap electrodes with a 1-cm diameter and 2-cm center-to-center spacing (Noraxon, Scottsdale, AZ, USA) were placed on the belly of the flexor digitorum superficialis (FD) and posterior deltoid (PD) muscle before starting the test. The SENIAM guidelines were followed for skin preparation, electrode placement, and orientation. Electromyographic signals were registered with a telemetric EMG system, which had a gain of 1000 Hz, a bandwidth (–3 dB) of 10 to 500 Hz, and a common mode rejection ratio > 85 dB. The signal was relayed to the computer via a 16-bit A/D converter (Myotrace 400, Noraxon, Scottsdale, AZ, USA). Only the concentric phase was included, and only the iEMG signal of the maximal repetition was chosen for subsequent statistical analyses. The period of activation was determined as the period where the signal was above a threshold of 15% of the maximum activity of that muscle during the test for at least 100 ms (Damasceno et al., 2014, 2015). The root mean square (RMS) of the EMG signal recorded during the MBboard-1RM test was normalized to the RMS recorded during the last muscle contraction measured during the specific warm-up protocol (i.e. load of 5 kg).
Statistical analysis
Data distribution was analysed by the Shapiro-Wilk test and the results showed a normal Gaussian distribution. Data are reported as mean and standard deviation (SD). RCG and CG data were compared by an unpaired t-test. The Pearson product-moment coefficient was used to determine the relationship between MBboard-1RM and climbing experience for the RCG. Intraclass correlation coefficient (ICC) was used to determine the reliability of the MBboard-1RM for the RCG during test and retest sessions, assuming an ICC value < 040 as poor, between 0.40 and 0.70 as fair, between 0.70 and 0.90 as good and > 0.90 as excellent (Coppieters et al., 2002). Statistical significance was set at p < 0.05. All analyses were performed using the SPSS program (version 13.0, Chicago, USA).
Results
Validity and reliability of MBboard-1RM
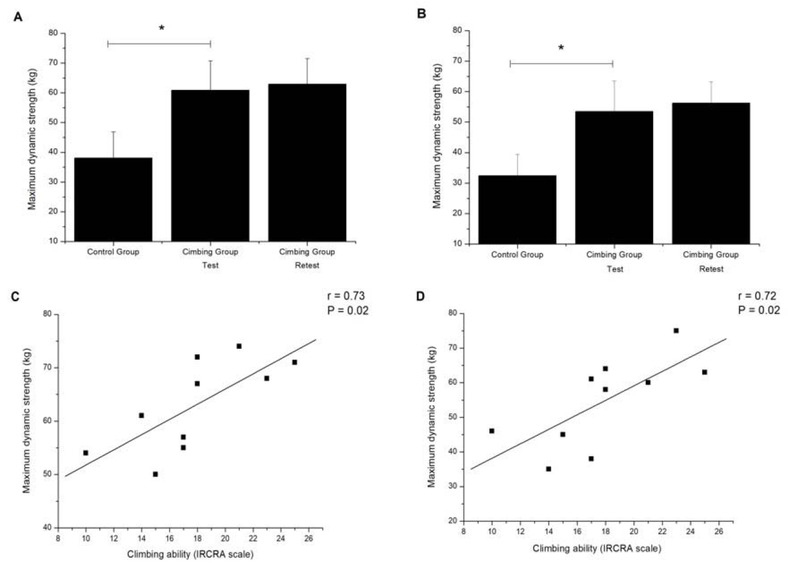
Figure 3 shows the maximum dynamic strength measured by the MBboard (i.e., test and retest MBboard-1RM) for both the CG and the RCG, as well as the correlation between MBboard-1RM and climbing ability self-reported by the RCG. The RCG had a superior performance in MBboard-1RM when compared with the CG for both dominant (p < 0.01, Panel A) and non-dominant (p < 0.01, Panel B) upper-limbs. There were significant Pearson product-moment correlations between MBboard-1RM performed on dominant (r = 0.73, p = 0.02, Panel C) and non-dominant (r = 0.72, p = 0.02, Panel D) upper-limbs with climbing ability. ICC analysis revealed good reliability between the trials for both dominant (ICC = 0.79, p = 0.01) and non-dominant (ICC = 0.85, p < 0.01) upper-limbs in RCG.
Figure 3
Maximum dynamic strength measured using the MBboard (Panel A: dominant upper-limb, Panel B: non-dominant upper-limb) and association between MBboard-1RM and climbing ability (Panel C: dominant upper-limb, Panel D: non-dominant upper-limb). Data are presented as mean ± SD. * Significantly higher than the control group (p < 0.05).
Surface electromyographic activity during MBboard- 1RM
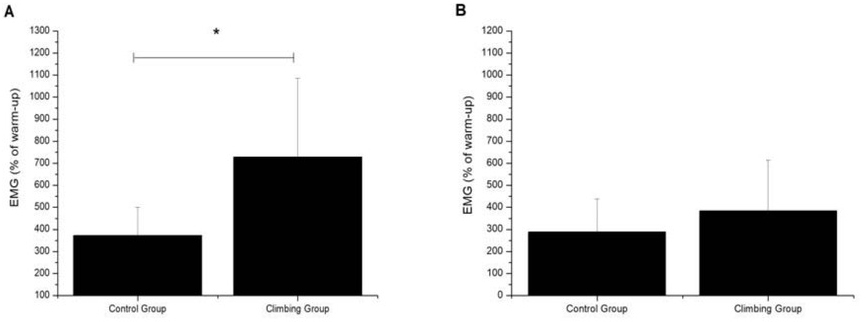
Figure 4 shows EMG activity for the flexor digitorum superficialis (panel A) and posterior deltoid (panel B) during MBboard-1RM evaluation. EMG activity for the flexor digitorum superficialis was significantly higher for the RCG (p < 0.01) when compared with the CG, while there were non-significant differences between the RCG and the CG (p = 0.11) in EMG activity for the posterior deltoid.
Discussion
The purpose of this study was to develop a low-cost and easy-to-build tool designed to evaluate maximal upper-limb strength in rock climbers in a specific way. Our main results revealed that: i) MBboard-1RM was able to discriminate between individuals with different climbing experience levels, ii) MBboard-1RM was significantly correlated with climbing ability self-reported by rock climbers, and iii) good reliability of MBboard-1RM was found when analysed within trials. Taken together, these findings suggest that the MBboard is a valid and reliable tool to assess rock climbing-specific upper-limb strength.
Previous studies have widely recommended the development of new tools for rock climbing-specific performance measurements (Giles et al., 2006; Sheel et al., 2004; Watts, 2004). To the best of our knowledge, this is the first study to develop a low-cost and easy-to-build tool (i.e., MBboard) to assist in the evaluation of upper-limb strength in rock climbers. The MBboard was designed in order to meet the specific upper body muscular demand of rock climbing which has been characterized by high-intensity isometric contraction of the forearms combined with dynamic whole-body movements (Limmer et al., 2019). Considering that there was no method universally accepted as gold standard for the measurement of maximal strength in rock climbers (Michailov et al., 2018), previous studies have adopted the strategy to obtain construct validity evidence of field and laboratory tests by comparison between individuals with different rock climbing experience and/or by association with climbing ability self-reported by rock climbers (Brent et al., 2009; Grant et al., 1996; López-Rivera and González-Badillo, 2019; Michailov et al., 2018). In the current study, the RCG presented superior MBboard-1RM performance when compared with the CG for both the dominant (p < 0.01) and the non-dominant (p < 0.01) upper-limb. Our results also revealed that MBboard-1RM was positively correlated with climbing ability, indicating that better rock climbers were able to produce higher values of MBboard-1RM. Collectively, these findings denote the construct validity evidence of the MBboard for the measurement of maximal upper-limb strength in rock climbers in a specific way.
Another interesting result of the present study was that EMG activity of the flexor digitorum superficialis had a similar response to MBboard-1RM performance, with the RCG showing higher values than the CG (Figure 3, panel A). In contrast, there was no significant difference between groups for EMG activity of the posterior deltoid (Figure 3, panel B). This is in accordance with previous results showing the importance of neuromuscular variables, such as finger flexors EMG activity, for rock climbing performance (Cutts and Bollen, 1993; Limonta et al., 2008; Magiera et al., 2013; Quaine et al., 2003; Vigouroux and Quaine, 2006). Vigouroux et al. (2015), for example, reported a significantly higher finger flexor muscles activation of rock climbers when compared with non-climbers. Deyhle et al. (2015) found a great reduction in digit flexion EMG activation after a fatiguing climbing task, suggesting that finger flexor muscle groups were one of the most recruited muscles for climbing on an overhanging wall. Taken together, these findings suggest that ability of the MBboard to assist in the assessment of rock climbing-specific strength may be related in part to the finger flexor muscles activation, probably reflecting the specific adaptations resulting from long-term practice of this sports discipline.
From the practical perspective, it is also important to determine the reliability before using a new performance test to accurately monitor and prescribe training protocols. A reliable test is one that has small changes in mean values, a small within-individual variation, and a high test-retest correlation (Stöggl et al., 2006). The reliability of performance tests can be statistically determined by different ways, with the ICC being considered one of the most appropriate statistical analysis for this proposal (Impellizzeri and Marcora, 2009). Although none of the rock climbers had used the MBboard before, our findings revealed good reliability of MBboard-1RM for both dominant (ICC = 0.79, p = 0.01) and non-dominant (ICC = 0.85, p < 0.01) upper-limbs. In the present study, we adopted only one familiarization trial in the experimental design before the experimental trials, which appears to be sufficient to mitigate the practice effects on MBboard-1RM performance. Therefore, this suggests that, using at least one familiarization session, it is possible to achieve good reliability of MBboard-1RM for detecting rock climbing-specific strength.
Some limitations of the present study should be recognized. First, when climbing a route or during a bouldering task, climbers have to use a wide variety of artificial handholds with different shapes and size to reach the top. This may impose different hand and finger positions to achieve optimal grip strength. Second, we were able to analyse only the unilateral seated cable row exercise, while climbing routes are typically built on artificial walls with different inclinations, which may require a wide variety of movements. In this respect, further studies are required to investigate the influence of other artificial handholds, finger positions, and upper body movements on the validity and reliability of the MBboard for detecting rock climbing-specific strength.
In conclusion, the findings of the current study provided construct evidence of validity and reliability of the MBboard for the measurement of rock climbing-specific strength. From the practical point of view, these findings open a new path for the use of the MBboard as a specific auxiliary tool for evaluation and prescribing strength based-training.